Patient Information
Our goal is to provide high-quality medical care and answer all your questions to ensure your experience is as comfortable and informative as possible. Here you’ll find answers to the most frequently asked questions – from clinic operations to procedure-related topics. If you don’t find the information you’re looking for, our team is always ready to assist you.

Patient Guide
Elite Clinic has a treatment funding agreement with the Estonian Health Insurance Fund (EHIF) for gynecology and infertility services.
If a patient with valid health insurance wishes to receive additional care services (i.e., comfort or premium services) beyond those covered
by EHIF, they may choose individual specialist care. The current price list for individual services is available [here].
For other medical specialties, as well as for patients without health insurance, our services are provided on a paid basis.
Yes, Elite Clinic offers free parking.
Elite Clinic is open:
Monday to Thursday: 8:00–19:00
Friday: 8:00–17:00
Every other Saturday: 10:00–14:00
The reception desk is open throughout the clinic’s working hours.
Opening hours may change during the summer period — updates will be shared on our website.
On working days preceding public holidays, the clinic closes earlier, in accordance with Estonian law.
The clinic is closed on public holidays.
Yes, you can. The nearest bus stops to Elite Clinic are Arhitekti and Ravila.
Bus lines 2 and 12 serve these stops. Both are just a short walk from the clinic.
Yes. Elite Clinic has a treatment funding agreement with the Estonian Health Insurance Fund, including for infertility treatment. This means
that patients with valid health insurance can receive infertility consultations and treatment at the expense of EHIF, paying only a visit
fee of either €20 or €5, depending on the specific situation.
Infertility procedures covered by EHIF are available until the woman reaches the age of 41.
For patients without health insurance, infertility treatment is self-funded.
If a patient wishes to use additional care or comfort services not included in EHIF-covered treatments, they have the option to choose
individual specialist care.
If you have previously visited Elite Clinic and wish to consult with a doctor or receive your test results, please send us an email at elite@elitekliinik.ee or call the clinic and provide your name, phone number, and the name of your doctor to the reception desk.
Your message will be forwarded to the doctor, who will contact you as soon as possible.
It is not recommended to visit a gynaecologist during menstruation.
For an initial infertility consultation, we recommend booking your appointment on day 3 to 5 of your cycle.
IUD insertion appointments are usually scheduled at the end of your period.
In general, a referral is required to see a specialist under the Estonian Health Insurance Fund (EHIF), except for visits to an ophthalmologist, gynaecologist, or psychiatrist.
At Tähe Private Clinic, EHIF-covered services are offered in the field of otorhinolaryngology (ENT), and a referral is required for an outpatient appointment.
At Elite Clinic, EHIF-covered services are provided in the fields of gynaecology and infertility treatment, and no referral is needed for outpatient appointments in these specialties.
For all paid services at our clinics, no referral is required.
No, the doctor will call you from the clinic’s official mobile number.
This number is only active while the doctor is at the clinic, and it cannot be used to reach the doctor outside clinic hours.
The clinic operates according to its regular schedule during the summer.
Collective vacation applies only to the surgical department and the embryology and andrology laboratories. During this time, no IVF procedures are performed.
The collective holiday usually lasts three weeks in July, possibly extending into August, and also includes the last week of December.
For detailed information, please contact the reception:
📞 +372 740 9930
📧 elite@elitekliinik.ee
Yes, we welcome patients regardless of their country of residence or insurance status.
All patients receive the necessary medical care on equal terms.
Payment is made at the reception after your appointment, based on the invoice provided by the doctor.
You can pay in cash or by card.
Tartu is easily accessible by plane, bus, car, and train.
By plane:
-Tartu Airport has direct flights from/to Helsinki. From the airport, the city center and Elite Clinic can be reached by taxi or public transport in about 15 minutes. Tallinn Airport has direct flights from/to different European cities.
By bus:
-There are frequent and comfortable bus connections from Tallinn, Riga, and other major cities.
By car:
-Tartu is about a 2–2.5 hour drive from Tallinn. Roads are well maintained, and free parking is available.
By train:
-There are regular train connections between Tallinn and Tartu.
-Starting from January 2025, you can also travel by train from Tallinn and Tartu to Latvia and Lithuania. The international train to Riga and Vilnius runs once a day and includes a transfer at Valga station.
If needed, our clinic staff will be happy to assist you with travel planning and local transportation.
Complaint Resolution Procedure
Complaint Resolution Procedure and Patient Satisfaction Surveys at AS Kliinik Elite and OÜ Tähe Erakliinik:
Patients may submit a complaint or provide feedback regarding the healthcare services or other matters at the clinic:
- using the form available in the clinic’s waiting areas and handing it to the secretary
- by mailing the same form or a free-form letter to: Sangla 63, Tartu
- by emailing the same form or a free-form message to: info@elitekliinik.ee
If you wish to receive feedback or a resolution to your complaint, please include your name and contact details in your message. A written response will be provided within two weeks.
To clarify and resolve the matter, submitted complaints/feedback will be forwarded to:
- issues related to nursing staff – Head Nurse Gerli Raieste
- issues related to medical treatment – Dr Andrei Sõritsa
- issues related to general organization – Quality Manager Malle Tiidelepp
If a complaint concerns a specific staff member, a written explanation will be requested from the person involved. Feedback will be given to the complainant, and internal measures will be implemented to prevent similar issues in the future.
The national system for ensuring the quality of healthcare services — including guidance on what to do if the service provided does not meet your expectations — is described in detail here: https://www.sm.ee/tervise-edendamine-ravi-ja-ravimid/ravi-ja-tervise-taastamine/tervishoiuteenuste-kvaliteet
Cancelling an Appointment and Failure to Attend
To ensure efficient organization of clinic and doctor schedules, patients must notify the clinic of their inability to attend an appointment or procedure at least 24 hours in advance via:
- Phone: +372 740 9930 (Monday to Thursday: 8:00–19:00, Friday: 8:00–17:00, every other Saturday: 10:00–14:00)
- Email: elite@elitekliinik.ee or info@elitekliinik.ee
If a patient fails to attend a scheduled specialist appointment without prior notice, they will be required to pay double the standard visit fee at their next healthcare service appointment (based on the Health Insurance Act § 70, clause 6).
Patient Satisfaction Surveys
Elite and Tähe Clinics conduct annually comprehensive patient satisfaction surveys.
Patient feedback on healthcare services and providers is vital for assessing the clinic’s performance and improving the delivery, quality, and content of care. This obligation is also outlined in the Minister of Social Affairs Regulation No. 128 “Requirements for Ensuring the Quality of Health Services”, which states that healthcare providers must, at least once a year, compile a summary of patient satisfaction, analyze and discuss the results, and implement necessary improvements.
If you would like information about the results of our patient satisfaction surveys in English, please feel free to contact us by email (info@elitekliinik.ee).
Patient Insurance
Starting from November 2024, mandatory liability insurance for healthcare providers — also known as patient insurance — took effect in Estonia.
For patients, this new system provides the right to claim compensation from the insurer if an avoidable health injury occurs due to a medical error after the law comes into force.
AS Kliinik Elite and OÜ Tähe Erakliinik have valid mandatory liability insurance with PZU Insurance as of 15 November 2024. For more information: PZU – Mandatory Liability Insurance for Healthcare Providers. https://pzu.ee/ariklient/tervishoiuteenuse-osutaja-kohustuslik-vastutuskindlustus/
Additional reading
Read More About Fertility and Infertility
Stress and Infertility
Stress is defined as any event that a person perceives as threatening or harmful. Stress can result in the heightened activity of many body organs. This increased activity is offset by hormones secreted by the adrenal glands and through the nervous system. Acute stress can result in increased heart rate, blood pressure, and respiration, as well as sweaty palms and cool, clammy skin. Chronic stress can also cause depression and result in changes in the immune system and sleep patterns.
Stress… causing Infertility
Although infertility is a highly stressful experience, there is very little evidence that infertility can be caused by stress. In rare cases, high levels of stress in women can change hormone levels and cause irregular ovulation. Some studies have sown that high stress levels may also cause fallopian tube spasm in woman and decreased sperm production in men.
Infertility…causing Stress
Research has shown that women undergoing treatment for infertility have a similar, and often higher, level of “stress” as women dealing with life-threatening illnesses such as cancer and heart disease. Infertile couples experience chronic stress each month, first hoping that they will conceive and then dealing with the disappointment if they do not.
Why Infertility is so stressful?
When diagnosed with infertility, many couples no longer feel in control of their bodies or their life plan. Infertility can be a major crisis because the important life goal of parenthood is threatened. Most couples are accustomed to planning their lives. Experience has shown that if they work hard at something, they can achieve it. With infertility, this may not be the case. Infertility testing and treatments can be physically, emotionally, and financially stressful. A couple’s intimacy is often reduced by the infertility experience, which further contributes to increased stress levels. Trying to coordinate medical appointments with career responsibilities can also increase pressures on infertile couples.
TIPS for stress reduction:
- Keep the lines of communication open with your partner.
- Get emotional support so you don’t feel isolated. Individual or couple counselling, support groups, and books on infertility can validate your feelings and help you cope.
- Learn stress reduction techniques such as meditation or yoga.
- Avoid excessive intake of caffeine and other stimulants.
- Exercise regularly to release physical and emotional tension.
- Have a medical treatment plan your and your partner are comfortable with.
- Learn as much as you can about the cause of your infertility and the treatment options available. Check your local library, bookstore, or the Internet for additional information on infertility.
Prediction of Fertility Potential in Female Patients
A woman’s reproductive potential declines with age. This is reflected in the decreased ability to conceive (become pregnant) and increase in the rate of spontaneous abortions (miscarriages).
Although fecundity (the ability to achieve a pregnancy that results in a live birth) decreases in all women as they age, the precise age when a woman can no longer conceive varies between individuals. Approximately one-third of couples in which the female partner is in age 35 or older will have problems with fertility. It is estimated that two-thirds of women will not be able to get pregnant spontaneously by the age of 40.
Several tests may be useful in assessing fertility potential in older patients. For those patients with poor fertility potential predictions, the use of donor eggs (egg donation) or embryos (embryo adoption) can be considered.
Day 3 levels of FSH, LH, and estradiol. The determination of blood concentrations of follicle stimulating hormone (FSH) and estradiol levels on menstrual cycle day 3 has been used to estimate fertility potential. Women with elevated levels of FSH and/or estradiol measurements on cycle day 3 have very poor pregnancy rates with both ovulation induction and assisted reproductive technologies (ART) such as in vitro fertilization (IVF). More recently, it has been shown that women with elevated blood levels of luteinizing hormone (LH) on cycle day 3 also have poor pregnancy outcomes with fertility therapy.
Clomiphene citrate challenge test.
This test entails the oral (by mouth) administration of 100 milligrams of clomiphene citrate on menstrual cycle days 5-9. Blood levels of FSH are measured on cycle day 3 and again on cycle day 10. Elevated blood levels of FSH on cycle day 3 or cycle day 10 are associated with very low pregnancy rates with both ovulation induction therapy and ART.
Response to gonadotropins.
Gonadotropins (Pergonal (R), Humegon (R), and Repronex (R)) are concentrated mixtures of FSH and LH or FSH alone (Fertinex (R), Follistim (R), or Gonal-F (R)), which are given as injections to stimulate the ovary to produce multiple eggs in preparation for various fertility therapies. The amount of gonadotrophins required to induce egg development increases with increasing chronological age. Patients requiring large amounts of gonadotropins to induce egg development generally have lower pregnancy rates with both ovulation induction therapy and ART.
Several laboratory methods are currently used to measure blood levels of FSH, LH, and estradiol. Measurement of these hormone levels may vary considerable depending upon the particular laboratory method used. Therefore, it may be difficult to compare blood levels of these hormones that are measured at different laboratories or by different laboratory techniques. It is important that normal and abnormal test values be based on the pregnancy rates achieved by women studied at a particular center using the same laboratory methods.
Planning an Effective Infertility Treatment Strategy
referred to Michael Kettel, M.D. and William Hummel, M.D
from San Diego Fertility Center
- Establish a Diagnosis
- The Infertility Evaluation
- Age and the Reproductive Process
- Formulating a Game Plan
- When to Move On
- When to Stop
- Conclusion
ESTABLISH A DIAGNOSIS
The normal menstrual cycle is a repetitive process which might be viewed as “reproductive failure.” As the normal physiologic intention of the menstrual cycle is to result in a pregnancy each and every time it occurs, menstrual bleeding might be viewed as failure of this process to occur. The hallmarks of the menstrual cycle include a dynamic coordination of the hypothalamic- pituitary-ovarian-endometrial axis to culminate in the release of a mature oocyte.
This mature oocyte must be successfully retrieved by the fimbriated end of the fallopian tube and made available for fertilization. In an independent process, sperm placed in the vagina at the time of intercourse must successfully survive the hostile environment of the vagina, enter the favourable confines of the cervical mucus and ultimately work themselves into the upper genital tract. The head of each sperm contains specific binding sites for the outer layer of the egg (zona pellucida). Once the sperm has bound to the zona pellucida then the fertilization process can occur. After ovulation, the egg lives for approximately 72 hours. Therefore, intercourse every other day around the mid cycle should successfully result in a condition in which fertilization can be maximized. Realizing the intricacies of this system, the normal fertility curve can be appreciated.
Cycle fecundity is a term used to describe the likelihood of a pregnancy occurring with each individual menstrual cycle. The human is a relatively inefficient reproducer and, in fact, the cycle fecundity is approximately 22%. If one views this fertility curve over time, successful reproduction is a result of repetitive attempts at this intricate fertilization process. Realizing, and keeping in perspective the normal fecundity curve can allow patients and physicians to embark in fertility treatments with realistic expectations.
INFERTILITY EVALUATION
The infertility evaluation consists of a variety of tests to document normal sperm, normal ovulation, fallopian tubal patency, normal endometrial environment, and a normal pelvis. There are multiple, controversial tests that have been proposed to evaluate the reproductive condition and identify particular pathologic disorders. Tests that fall into this controversial category including the following: post coital test, late luteal phase endometrial biopsy, antisperm antibody determinations, penetration tests, and serial ultrasounds to determine the luteinized-unruptured-follicle syndrome. All of these controversial tests have relatively poor sensitivity and specificity and, as a result, are fraught with false negatives and false positives. Using these tests, therefore, should be approached with caution. Certainly many pregnancies have resulted in couples whom antisperm antibodies have been identified…
The diagnosis of “unexplained infertility” then becomes a diagnosis of exclusion. It reflects our lack of understanding of the reproductive process and includes couples that are normal as well as couples who may have subtle defects in the reproductive process. The treatments for unexplained infertility places a couple in a relatively favourable prognostic category. When viewed with other common causes of infertility, unexplained infertility often results in both treatment dependent and treatment independent success.
AGE AND THE REPRODUCTIVE PROCESS
Most people are aware that increasing maternal age leads to a decline in fertility. In fact, this decline occurs fairly acutely after the age of 37 and continues to decline up through the menopause. In almost any arena in which age is evaluated, advancing age leads to a decline in either treatment success or ultimate pregnancy outcome. With advancing maternal age increases also miscarriage rate and increase chromosomal abnormalities . Once a pregnancy has successfully entered the second trimester, it does not appear that other pregnancy risks are increased. One test which can offer some insight into this aging process is the “day 3” FSH. FSH is the pituitary hormone which is primarily responsible for folliculogenesis. As such, an increasing day 3 FSH reflects ovarian resistance to ovulation. In some studies the day 3 FSH has been shown to be a better predictor of pregnancy success than chronologic age. A day 3 FSH of greater than 25 mIU/mL places the woman in a relatively poor prognostic category whereas a day 3 FSH of less than 15 mIU/ml places the woman in a good prognostic category. It must be emphasized that the day 3 FSH value varies from cycle to cycle and that a singled isolated, elevated day 3 FSH is not the final bad signal for a woman considering pregnancy.
FORMULATING A GAME PLAN
The treatment of many causes of infertility revolves around a concept to increase cycle fecundity. Cycle fecundity is the likelihood of a pregnancy resulting in any given menstrual cycle. Treatments that increase cycle fecundity can be applied to a multitude of pathologic conditions. These treatments accelerate the “fertility curve” and may improve the otherwise protracted curve of patients with unexplained infertility. There are three basic techniques to increase cycle fecundity:
- The first technique is intrauterine insemination(IUI). Intrauterine insemination involves a process that improves the timing of insemination to ovulation, increase the number of motile sperm that reach the fallopian tubes and may increase the number of capacitated sperm that reach the upper genital tract.
- The second technique to increase cycle fecundity is superovulation. Superovulation requires the use of fertility drugs. Clomiphene citrate, human menopausal gonadotropins (Pergonal, Humegon, hMG) or rec(recombinant)FSH (Gonal-F, Puregon) have been used to induce a condition of superovulation. When these drugs are prescribed, the expected result is an increase in the number of ovulated eggs per cycle to result in an increase in the likelihood of fertilization occurring. Fertility drugs may also increase the efficiency of folliculogenesis and may improve subtle luteal phase insufficiencies.There is now a body of literature which hasexamined each of these techniques in unexplained infertility. It appears that intrauterine insemination and clomiphene citrate do a relatively poor job of increasing cycle fecundity when used alone. It is the combination of clomiphene citrate plus intrauterine insemination which results in an increase in cycle fecundity. The use of hMG or recFSH either alone or in combination with intrauterine insemination has been shown to increase cycle fecundity. Overall, the best results are seen when these drugs are used together with IUI.
- The third technique that results in an increase in cycle fecundity are assisted reproductive technologies, which include a variety of procedures including IVF-ET, ICSI-ET.
WHEN TO CHANGE TREATMENT SCHEME
Each treatment cycle should be viewed as an independent event. This means that if the first cycle fails, the next cycle has an equal chance of working! this cycle independence holds true for each type of treatment for three cycles of treatment. If you examine the clinical efficacy of a given treatment protocol, the cumulative pregnancy should be viewed as the likelihood of conception within a reasonable time frame, approximately 3-4 cycles, and NOT after only one attempt.
When deciding when to move from one treatment protocol to another, it is important to review what has been learned from the preceding treatments. Did the ovaries respond appropriately? Did the endometrium reach a target thickness? Did the follicles release the eggs? Were the hormone levels correct? By examining the response to treatment the patient and physician can decide when it is appropriate to move from one treatment protocol to another.
By and large, if a treatment is going to work, it will be effective within three cycles. The majority of success occur during the first three attempts and this presents a reasonable interval in which to schedule a re-evaluation consultation with your physician. Before this visit, the patient must re-evaluate their feelings and comfort zone about treatments. It is interesting to observe the changes in a couple’s comfort zone as they experience successes and failures with differing treatments. A couple who first thought they would not possibly consider artificial insemination may seriously look at IVF after a few cycles of hMG injections!
WHEN TO STOP TRYING…
The decision to stop treating is probably one of the most difficult decisions faced by any couple who struggles with infertility. A sense of when to stop and when to continue can be reached if a couple has a firm grasp on their objectives. For instance, one couple may have as their goal to have a baby in their home and are willing to consider adoption or egg donation as a route to achieve this goal, whereas another couple is not at all interested in this approach and have decided that if they cannot conceive using their own egg/sperm they would not have children. Very personal choices that differ from couple to couple.
Unfortunately, your doctor may not help much with this decision. Remember…it is the doctor’s job to think of alternatives and choices for you to consider. It is your job to decide which choice is best for you. One couple may enthusiastically proceed with egg donation IVF whereas another stops short of laparoscopy to correct endometriosis.
CONCLUSION
- Establish a diagnosis
- Begin treatment at an appropriate level
- Evaluate a treatment plan at three cycle intervals
- Keep an open mind and long-term goals in perspective
A sexually active woman between the ages of 20 and 30 has a monthly pregnancy probability of approximately 25%. This means that out of every ten women trying to conceive, about nine will successfully become pregnant within a year.
However, one in ten will not conceive – meaning these women are either infertile or have reduced fertility. Clinically, infertility is generally defined as the inability to achieve pregnancy after one year of regular, unprotected intercourse.
Fortunately, many women facing fertility challenges can successfully achieve pregnancy using assisted reproductive technologies (ART), such as IVF. Additionally, a variety of other medical treatments and diagnostic evaluations are available for couples to explore prior to pursuing artificial insemination. It is also quite common for a woman who has previously participated in a fertility program to later conceive naturally, despite having faced years of unexplained infertility in the past.
Through comprehensive clinical diagnostic testing, the underlying cause of infertility can usually be identified. The cause remains unexplained in about 20% of cases, and even within this group, couples are frequently able to achieve a successful pregnancy. Statistically, female factor infertility accounts for approximately 40% of cases, while male factor infertility accounts for another 40%.
To determine the specific cause of fertility challenges, standard diagnostic evaluations include:
- For women: Ovulation tracking, hormone level testing, and evaluation of fallopian tube patency.
- For men: Assessment of sperm production—including sperm count, motility, and morphology—which requires a comprehensive semen analysis.
Female Infertility Causes
-
Hormonal imbalances: Endocrine disorders that disrupt the development of ovarian follicles or prevent the release of a mature egg from the ovary (ovulatory dysfunction or anovulation).
-
Damaged or blocked fallopian tubes: Tubal factor infertility that prevents the egg and sperm from meeting or stops a fertilized embryo from reaching the uterus.
-
Endometriosis: A condition where tissue similar to the lining of the uterus grows outside the uterine cavity, causing inflammation and damaging neighboring reproductive organs.
-
Hostile cervical mucus: Abnormally thick cervical mucus that acts as a barrier, preventing sperm from surviving and passing into the uterus.
Male Infertility Causes
-
Low sperm count (Oligozoospermia): A healthy sperm count typically contains at least 15 to 20 million sperm per milliliter of semen. Counts below this threshold are considered a factor in reduced male fertility.
-
Poor sperm motility (Asthenozoospermia): The sperm lack the progressive movement required to travel through the cervix and reach the egg in the fallopian tubes.
-
Abnormal sperm shape (Teratozoospermia): Structural irregularities prevent the sperm from penetrating the outer layer of the egg or successfully completing fertilization.
-
Azoospermia: The complete absence of sperm in the ejaculate, which can result from a failure in sperm production (testicular failure) or a blockage in the reproductive ducts (obstructive azoospermia).
-
Sexual dysfunction: Difficulties during intercourse, such as ejaculatory dysfunction or erectile dysfunction (impotence).
The Role of Assisted Reproduction
Guidelines for Semen Analysis (Sperm Test)
-
Abstinence window: The male partner must abstain from ejaculation for 2 to 7 days prior to the test.
-
Sample collection: The semen sample is collected via masturbation in a private room directly at the laboratory facility to ensure optimal sample processing.
Advanced Male Fertility Investigations
Diagnostic Examinations
Gynaecological Ultrasound
-
Transabdominal Ultrasound: Performed by moving a transducer across the lower abdomen. This approach requires a full bladder to optimize imaging.
-
Transvaginal Ultrasound: Performed by gently inserting a specialized probe into the vagina. This is the preferred method in gynecology as the shorter distance allows for significantly clearer, high-resolution images of the pelvic structures. This approach requires an empty bladder.
HyCoSy (Hysterosalpingo-Contrast-Sonography)
-
Procedure: A speculum is placed to visualize the cervix, and a thin, flexible catheter with a small retaining balloon is gently inserted. After removing the speculum, a safe contrast medium is introduced into the uterine cavity via the catheter. A transvaginal ultrasound probe is then used to track the contrast fluid as it fills the uterus, travels through the fallopian tubes, and spills out from the fimbriated ends (the uterine horns).
-
Duration & Comfort: The procedure takes about 20 minutes. No anesthesia is required, though mild, temporary cramping may occur, which can be managed with over-the-counter pain relievers before or during the session. Patients must empty their bladder prior to the procedure.
-
Advantage: It combines structural uterine screening with tubal patency testing in a single outpatient visit without exposing the patient to X-ray radiation.
Hysteroscopy
-
Procedure: A thin, fiber-optic telescope (hysteroscope) is guided through the vagina and cervix into the uterine cavity, providing a clear, illuminated view on a monitor. Upon removal, an endometrial biopsy (tissue sample) is typically taken to verify if the lining matches the expected phase of the patient’s menstrual cycle.
-
Treatable Conditions: Uterine polyps, uterine septums (a congenital tissue band dividing the cavity), and uterine fibroids (myomas).
-
Anesthesia & Recovery: Performed as a day-case procedure under general or local anesthesia, lasting 20 to 40 minutes. Post-procedure, patients may experience mild discomfort and mild cramping manageable with pain medication. Most patients return to normal activities the same day; if operative corrective surgery is performed, a few days of home rest are recommended.
Surgical Treatments for Female Infertility
Laparoscopy
-
Procedure: Under general anesthesia, a small incision is made near the navel, and carbon dioxide ($CO_2$) gas is introduced into the abdomen to separate the organs and optimize visualization. A fiber-optic laparoscope is inserted, and a second micro-incision may be made for a secondary probe to safely manipulate tissues.
-
Tubal Patency Dye Test: To test for blockages, a colored dye can be injected into the uterus through the cervix. If the fallopian tubes are open, the dye will be seen flowing through them and exiting into the pelvic cavity.
-
Duration & Recovery: The procedure takes approximately 20 minutes. Post-operative effects include mild pelvic discomfort and bloating from residual gas. Displaced gas near the diaphragm may cause temporary shoulder pain, which responds well to analgesics. Patients typically resume normal daily routines within 2 to 3 days.
Adhesiolysis
-
Procedure: Performed under general anesthesia. It is ideally completed laparoscopically, though severe, extensive cases may require a conventional laparotomy (abdominal incision). Specialized microsurgical instruments are used to carefully divide the tissue bands.
-
Recovery: Following a laparoscopic approach, discomfort is mild and easily managed with analgesics; patients are discharged the same or next day, returning to full activity within a week. A conventional laparotomy requires up to 5 days of hospitalization and a recovery window of up to 6 weeks.
-
Prognosis: Because adhesions can recur to varying degrees in some patients, couples are generally advised to try to conceive within one year following the surgery.
Salpingostomy
-
Procedure: Under general anesthesia, any restrictive scar tissue covering the end of the fallopian tube is meticulously cleared. The tube is then opened, and its edges are delicately folded back and secured to ensure it remains permanently open. The surgery lasts 40 to 60 minutes and is performed either laparoscopically or via a conventional abdominal incision.
-
Recovery: Prophylactic antibiotics are administered post-op to prevent subsequent infections that could cause re-scarring. Pain is managed effectively with analgesics. Laparoscopic patients go home the same day and recover within a week, whereas conventional surgery requires a 5-to-7-day hospital stay and up to 6 weeks of recovery.
-
Success Rates: While surgical opening of the tubes is successful in up to 80% of cases, the subsequent functional pregnancy rate is approximately 20% due to potential underlying microscopic damage to the inner cilia of the tubes.
Tubal Reversal (Reversal of Sterilization)
-
Preparation: The first step is to determine the length of the functional tube sections and locate the occlusion. This is assessed via a HyCoSy ultrasound or a hysterosalpingography (HSG) X-ray.
-
Procedure & Recovery: Performed under general anesthesia via laparoscopy or a mini-laparotomy. Post-operative discomfort is successfully managed with pain medication. Laparoscopic patients are discharged on the day of surgery and recover within a week. Conventional open approaches require 4 to 6 days of hospitalization and a 4-to-6-week recovery period.
-
Timeline: Couples are recommended to actively try to conceive within 6 to 12 months post-surgery, as long-term healing can sometimes trigger new scar tissue formation that could re-block the tubes.
Polycystic Ovary Syndrome (PCOS) Treatments
-
Medical Management: Aims to restore endocrine balance and induce ovulation. Medications like clomifene citrate work by modulating estrogen feedback, which increases the secretion of Follicle-Stimulating Hormone (FSH). Elevated FSH levels trigger healthy follicle maturation and subsequent ovulation.
-
Surgical Management (Ovarian Drilling / Diathermy): If medical management is unsuccessful, laparoscopic ovarian drilling is an option. Under general anesthesia, a laparoscope is used to view the ovaries, and a laser or specialized electrocautery (diathermy) probe applies precise local heat to puncture the ovarian cortex. This reduces hormone-producing tissue, lowers androgen levels, and helps restore regular ovulatory cycles. The procedure takes roughly 30 minutes, and patients return to regular activity within 2 to 3 days.
Surgical Treatments for Male Infertility
Varicocele Ligation
-
Procedure: Performed under general anesthesia, taking approximately 30 minutes. It can be executed as a day-case laparoscopic procedure or via conventional open surgery. The surgeon identifies the dilated veins and either ligates (ties them off) or injects a sclerosing solution to close them.
-
Recovery & Success Rates: Post-operative discomfort is mild and managed with standard pain medication. Varicocele ligation successfully improves sperm count, motility, and morphology parameters in 40% to 60% of patients.
Vasectomy Reversal (Vasovasostomy)
-
Procedure: Performed under general anesthesia and can last over an hour. The surgeon makes an incision in the scrotum or lower groin to locate the severed ends of the vas deferens on both sides. Using specialized multilayered microsurgical techniques (vasovasostomy), the pathways are meticulously reconnected to allow sperm to pass from the testes into the urethra for ejaculation.
-
Recovery: Patients return home the same day. Strenuous physical exertion must be avoided during the immediate post-operative days, with full recovery achieved within 1 to 2 weeks. Mild soreness is managed with analgesics.
-
Follow-up & Success: A semen analysis is scheduled three months post-surgery to evaluate the return and quality of sperm in the ejaculate. While anatomical success (sperm returning to the semen) is achieved in 70% to 80% of cases, successful natural conception depends heavily on the time elapsed since the original vasectomy. A longer interval increases the risk of permanent sperm quality decline or the development of anti-sperm antibodies.
-
Sperm Cryopreservation Backup: If cryopreservation facilities are available at the clinic, sperm can be harvested directly during the surgical procedure and frozen. If post-operative semen quality is insufficient for natural conception, this frozen backup can be utilized in assisted reproductive treatments like IVF or ICSI.
-
Ovulation Induction (OI)
-
In Vitro Fertilization (IVF)
-
Intrauterine Insemination with Donor Sperm (IUI-D / AID)
-
Intrauterine Insemination with Partner’s Sperm (IUI-H / AIH)
-
Oocyte (Egg) Donation combined with IVF
-
Intracytoplasmic Sperm Injection (ICSI)
-
Assisted Hatching (AH)
-
Testicular Sperm Aspiration (TESA)
-
Microepididymal Sperm Aspiration (MESA)
Ovulation Induction (OI)
-
Indications: This protocol is highly effective for women experiencing endocrine disorders or Polycystic Ovary Syndrome (PCOS).
-
Monitoring: To optimize the cumulative pregnancy rate and mitigate the risk of multiple pregnancies or ovarian hyperstimulation, response to treatment is closely monitored via transvaginal ultrasound and tracking follicle growth.
-
Success Rates: The average clinical pregnancy rate per treatment cycle ranges between 15% and 25%.
In Vitro Fertilization (IVF)
The General IVF Protocol:
-
Controlled Ovarian Hyperstimulation: A customized medication regimen is administered to stimulate the maturation of multiple ovarian follicles.
-
Cycle Monitoring: Follicle growth is carefully tracked using transvaginal ultrasound examinations (typically 2 to 3 times per cycle) and blood serum hormone assays to tailor medication dosages and prevent severe side effects.
-
Oocyte Retrieval (Egg Collection / Follicular Puncture): Mature eggs are harvested from the ovarian follicles via a minimally invasive ultrasound-guided procedure.
-
Sperm Collection: The male partner provides a fresh semen sample on the day of egg retrieval, or a previously cryopreserved sample is prepared.
-
Insemination: Collected mature eggs and processed, high-motility sperm are co-incubated overnight in a controlled laboratory environment.
-
Fertilization Assessment: The following day, microscopic evaluation confirms the presence of successful fertilization.
-
Embryo Transfer: One (or a maximum of two) high-grade embryo is gently transferred into the patient’s uterus under transvaginaal ultrasound guidance.
-
Embryo Cryopreservation: Any remaining high-quality embryos are safely vitrified (frozen) for future use.
-
Pregnancy Confirmation: Follow-up clinical screening and quantitative hCG testing are performed to track early pregnancy status.
Intrauterine Insemination (IUI)
IUI with Donor Sperm (IUI-D / AID)
IUI with Partner’s Sperm (IUI-H / AIH)
The General IUI Protocol:
-
Mild Ovarian Stimulation: A gentle medication course is used to promote the maturation of 2 to 3 follicles.
-
Follicle Monitoring: Progress is monitored 2 to 3 times per cycle via transvaginal ultrasound, combined with targeted hormone assays to optimize timing and ensure safety.
-
Ovulation Tracking: Assessment of basal body temperature and specialized ovulation prediction kits are utilized to identify the precise fertile window.
-
Sperm Processing: On the day of ovulation, the semen sample is washed and processed to isolate the highest quality, motile sperm.
-
Insemination: The concentrated sperm sample is transferred into the uterine cavity on the exact same day.
-
Follow-up: Clinical tracking is conducted to confirm successful implantation and pregnancy.
Intracytoplasmic Sperm Injection (ICSI)
ICSI with Surgical Sperm Retrieval (MESA/TESA)
-
MESA (Microepididymal Sperm Aspiration): Harvesting sperm directly from the epididymis.
-
TESA (Testicular Sperm Aspiration): Extracting sperm tissue directly from the testes.
The General ICSI Protocol:
-
Controlled Ovarian Hyperstimulation: Customized medication protocols are used to induce multiple follicle development.
-
Cycle Monitoring: Ultrasound scans and hormone level checks ensure safety and individualize dosing.
-
Oocyte Retrieval: Mature eggs are collected from the follicles.
-
Sperm Procurement: Sperm is obtained via fresh ejaculation or through surgical TESA/MESA extraction.
-
Micromanipulation (Injection): Mature eggs are denuded (cleared of outer cumulus cells), and one healthy sperm is carefully injected into each viable oocyte under a microscope.
-
Fertilization Verification: Microscopic evaluation the following day assesses fertilization progress.
-
Embryo Transfer: One or two high-grade embryos are transferred into the uterine cavity.
-
Vitrification: Remaining viable blastocysts/embryos are cryopreserved.
-
Pregnancy Care: Implantation is monitored through post-transfer diagnostics.
Embryo Transfer Procedure
Post-Transfer Care and Luteal Support:
-
Hormonal Support: For the subsequent two weeks, the patient receives luteal phase support to promote uterine receptivity and support implantation. This consists of either targeted hCG injections or daily vaginal progesterone administrations.
-
Embryo Banking: All additional viable embryos can be cryopreserved and securely stored for up to seven years, allowing for future Frozen Embryo Transfer (FET) cycles without the need for repeated ovarian stimulation.
-
Lifestyle Guidance: Patients can immediately resume their daily routines. However, during the post-transfer window, it is highly recommended to avoid sexual intercourse, refrain from lifting heavy objects over 10 kilograms, and avoid hot baths, saunas, or steam rooms.
Surgical Sperm Retrieval: TESA and MESA
-
TESA (Testicular Sperm Aspiration): A procedure where sperm or tissue samples are collected directly from the testes using a fine needle.
-
MESA (Microepididymal Sperm Aspiration): A procedure where sperm is harvested from the epididymis, often performed microsurgically.
Psychological Stress and Treatment Failure
Multiple Gestations (Multiple Pregnancy)
Ovarian Hyperstimulation Syndrome (OHSS)
Spontaneous Abortion (Miscarriage)
Required Screenings for the Male Partner
| Diagnostic Test | Validity Period |
|
Semen Analysis (Sperm Test)
Can be performed at the Elite Clinic andrology laboratory.
|
6 Months |
|
Infectious Disease Serology Panel:
* Treponema pallidum (Syphilis) antibodies
* HIV-1 & HIV-2 antibodies/antigens
* HBsAg (Hepatitis B surface antigen)
* HBcAb (Hepatitis B core antibody)
* Anti-HCV (Hepatitis C antibodies)
|
3 Months |
|
Sexually Transmitted Infection (STI) Screen via PCR:
* Neisseria gonorrhoeae
* Chlamydia trachomatis
* Trichomonas vaginalis
|
3 Months |
Required Screenings for the Female Partner:
| Category | Diagnostic Test | Testing Window | Validity Period |
| Infectious Diseases |
Serology Panel:
• Treponema pallidum (Syphilis) antibodies
• HIV-1 & HIV-2 antibodies/antigens
• HBsAg (Hepatitis B surface antigen)
• HBcAb (Hepatitis B core antibody)
• Anti-HCV (Hepatitis C antibodies)
|
Any day | 3 Months |
| STIs |
Screening via PCR:
• Neisseria gonorrhoeae
• Chlamydia trachomatis
• Trichomonas vaginalis
|
Any day | 3 Months |
| General Health | Complete Blood Count (CBC) | Any day | 3 Months |
| General Health | Blood Group & Rh Factor (ABO/Rh typing) | Any day | Lifetime |
| Cervical Health | Pap Smear (Cervical Cytology) | Outside of menstruation | 24 Months |
| Coagulation | APCR Test (Activated Protein C Resistance) | Any day | Lifetime / Once |
| Ovarian Reserve |
FSH (Follicle-Stimulating Hormone)
LH (Luteinizing Hormone)
|
Cycle Days 3–5
(Early Follicular Phase)
|
6 Months |
| Endocrine / Thyroid |
TSH (Thyroid-Stimulating Hormone)
Prolactin (PROL)
Total Testosterone
|
Any day
(Fasting morning blood draw required)
|
6 Months |
Pioneer Milestones of Our Medical Team:
-
August 1995: The birth of the first IVF (In Vitro Fertilization) baby in Estonia.
-
July 1996: The birth of the first Estonian baby achieved using a donated oocyte (egg donation).
-
September 1996: The birth of the first baby achieved using embryo donation.
-
March 1997: The birth of the first baby conceived via IVF using cryopreserved donor sperm.
-
June 1997: The birth of the first baby resulting from a frozen-thawed embryo transfer (FET) processed entirely within our own IVF laboratory.
-
1998: The birth of our first baby achieved via ICSI (Intracytoplasmic Sperm Injection) micromanipulation technology.
-
2001: The birth of the first baby achieved using Assisted Hatching (AH) laboratory techniques.
-
2002: The birth of the first baby achieved following our own surgically performed TESA (Testicular Sperm Aspiration) extraction combined with an ICSI procedure.
IVF and Embryo Transfer Coverage via Tervisekassa
-
Outpatient Fees: The patient is only required to pay a standard co-payment of either €5 or €20 for the initial consultation (these prices apply to patients with valid Estonian health insurance). All subsequent diagnostic evaluations, laboratory tests, and medical procedures within the treatment cycle are fully funded by Tervisekassa. There are no hidden or additional out-of-pocket costs for these services.
-
Medication and Reimbursements: Necessary fertility medications are prescribed by our specialists and purchased by the patient directly from the pharmacy. Patients are entitled to drug reimbursements in accordance with the Artificial Insemination and Embryo Protection Act (for detailed guidelines, please refer to the section: IVF Medication Reimbursement).
Lisalugemist raseduse teemal
Rasedusekalender
Raseduskalendri koostamisel on kasutatud väljaannet “Rasedus. Lapse sünd. Vastsündinu.”
Loode:
Umbes millimeetrisuurune munarakk on kinnitunud emaka limaskesta külge.
Hakkab moodustuma platsenta.
Hakkavad arenema soolestiku, kopsude ja närvisüsteemi alged. Osa rakke hakkavad moodustama nahka, lihaseid ja veresooni.
Naine:
Naine võib tunda end tavapärasest enam väsinuna ja kannatada peavalude all.
Mees:
Ühiselt elustiili tervislikumaks muutmine (toitumisele, liikumisele tähelepanu pööramine, suitsetamisest loobumine). Mees saab pakkuda emotsionaalset tuge ja praktilist abi igapäevastes toimingutes.
Uuringud:
Kõige varasem raseduse tuvastamise viis on vereanalüüs, millega määratakse platsenta eritatava kooriongonadotropiini (hCG) taset veres.
Vereanalüüs on mõnevõrra täpsem kui uriinitest. Sellega on võimalik rasedust kindlaks määrata umbes 10 päeva pärast viljastumist/embrüo siirdamist. Elite kliiniku üldlaboris saab vereanalüüsi teha ilma saatekirjata.
Loode:
Ultraheliuuringul on loode nähtav. Hakkab moodustuma loote selgroog ning ajul on moodustunud kaks sagarat. Lootel hakkavad arenema käed, jalad ja nägu. 8. nädalal on lootel moodustunud kõik peamised siseorganid. Süda lööb korrapäraselt. Loode on umbes 4 sentimeetrit pikk. Kuni 14.
nädalani mõõdetakse lapse pikkust peast seljani (CLR).
Naised:
Mõnel naisel võivad rinnad muutuda tundlikumaks kui tavaliselt ning tekkida vajadus sagedamini urineerida. Võib tekkida iiveldus. Naine võib tunda väsimust. Rinnanibude rasunäärmed võivad olla muutunud nähtavaks ja kombates tuntavaks. Tupevoolus võib suureneda, sellel rasedusperioodil on see normaalne. Kui naine vajab nõustamist ja ehk ka toitumisharjumuste muutmist, siis Elite kliinikus saab pöörduda toitumisnõustaja poole enda vajadustele vastavate soovituste saamiseks.
Mehed:
Mees saab pakkuda emotsionaalset tuge ja praktilist abi igapäevastes toimingutes. Oluline on ka julgustav ja positiivne suhtumine, sest rasedusega kaasneb naise jaoks sageli ärevus ja mure nii lapse kui enda tervise pärast. Soovi korral ja võimalusel võib käia koos arsti või ämmaemanda vastuvõtul. Kuna iga naine on eriline ja iga inimese vajadused on erinevad, on avatud suhtlus sel perioodil eriti tähtis.
Uuringud:
Rasedust saab tuvastada koduse rasedustestiga. Emakaõõnes saab rasedust diagnoosida 6. rasedusnädala alguses (5+). 6.-7. rasedusnädalal saab ultraheliuuringu abil tuvastada loote südametöö ja välistada emakaväline ja peetunud raseduse. Varajane ultraheli (6.-7. nädalal) on oluline ka embrüo väärarengute diagnostikas. Esimesel visiidil teostatakse järgmised analüüsid – vereanalüüs, analüüsid suguteedest, uriiniproov.
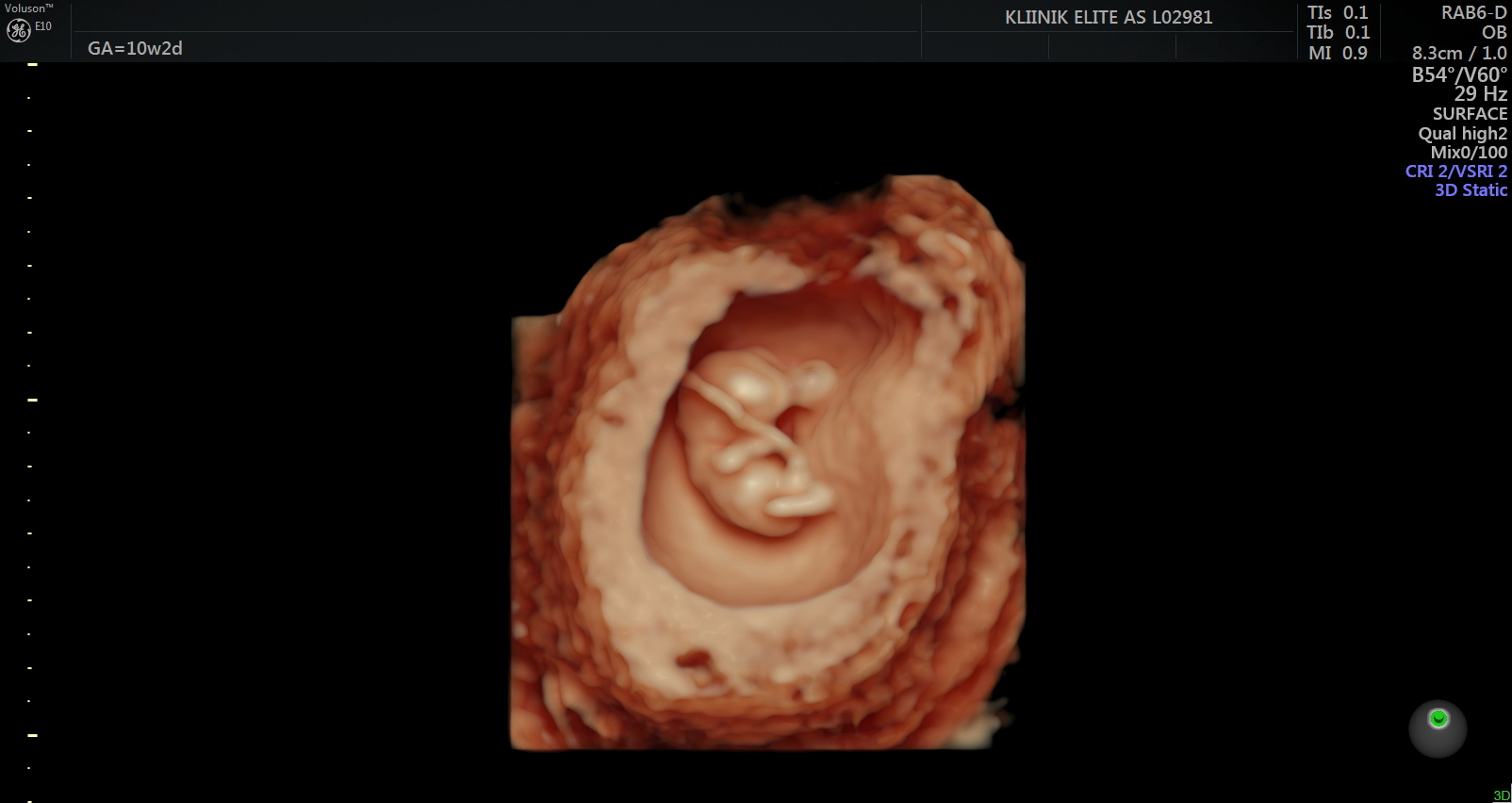
Loode:
Loote sõrmed ja varbad on sel ajal eristatavad. Pea moodustab peaaegu poole loote suurusest. Võrreldes 7. nädalaga on 10. nädalal loote kaal kahekordistunud. Kujunema hakkavad sõrme- ja varbaküüned. 11. nädalaks on moodustunud loote munandid või munasarjad. Loode suudab avada suud ning keel on välja arenenud. Välised suguelundid on nähtavad, kuid ultraheliuuringu käigus on neid veel keeruline eristada. Sel perioodil saab soo tuvastada Panorama ja Nifty testiga. 12. nädalal on lootel silmalaud. Loode liigub emakas ringi, kuid naine seda ei tunne. 12. nädalal kaalub loode umbes 25 grammi ja tema jala pikkus on 1 sentimeeter. Loode võib neelata väikestes kogustes lootevedelikku. 13.
nädalaks on lootel olemas kõik luud.
Naised:
Mõnikord ei soovi naised olla raseduse ajal seksuaalvahekorras. Kui arst või ämmaemand ei ole andnud juhiseid seksuaalvahekorrast loobuda, siis on see lubatud ja loodet ei kahjusta. Sel perioodil võivad igemed veritseda, võib esineda ninaverejooksu. Emakas on laienenud ja selle suurust võib võrrelda apelsiniga. Rinnad tunduvad raskematena kui varem. Kui naisel esines iiveldust, siis 11. nädalal hakkab see taanduma. Raseda naise vere hulk on suurenenud ja suureneb veelgi kuni lapse sünnini. Naise kehakaal hakkab tõusma.
Mehed:
Mehe toetus sel perioodil on eriti oluline, kuna esimest trimestrit peetakse riskantseks ajaks. Ligikaudu 10-20% rasedustest katkeb ja
enamasti juhtub see enne 12. nädalat. Ärevust lisab erinevate uuringute vastuste ootamise aeg. Naine vajab sageli tuge nii emotsionaalselt kui füüsiliselt. Elite kliinikus saab soovi ja vajaduse korral pöörduda psühholoogi vastuvõtule, kes nõustab, kuidas ülemäärase ärevusega toime tulla.
Uuringud:

Loode:
Lootel on juuksed. Ta liigutab oma pead, käsi ja jalgu. Jalad on kätest pikemad. Kui lapsel on tumedate juuste geenid, siis hakkavad need praegu tootma tumedat pigmenti.
Laps teeb rinnaga üksikuid hingamisliigutusi. Väikeaju ja selgroog on moodustunud. Loode on 16 sentimeetri pikkune ja kaalub umbes 130 grammi.
Loote liigutused toimuvad võpatustena. Tal on nii aktiivseid kui ka passiivseid perioode. Pea veresooned on juba nähtavad. Loode saab pead pöörata. Käed ulatuvad kokku.
Naine:
Naine ei pruugi olla enam nii väsinud, ka muud sümptomid võivad leeveneda. Lapseootel naine võib märgata tumedat joont kõhu keskel, nabast allpool, mis kaob pärast lapse sündi. Emakas on greibisuurune ja algab kõhu märgatav kasv. Naise südame maht on suurenenud. Mõned naised täheldavad seda kui südame pekslemist, ent see on ohutu. Võib esineda torkivat valu kõhupiirkonnas, see on märk emakalihaste venimisest.
Mees:
Mees saab toetada partnerit nii füüsiliselt kui emotsionaalselt. Kuna naine tunneb end tavaliselt sel ajal hästi, võiks see olla sobiv aeg, et planeerida ühist koosveedetud aega.
Seksuaalsel teel levivate infektsioonide avastamisel on vajalik raseda ja tema partneri ravi ning ravijärgne korduv kontroll.
Uuringud:
Vererõhu mõõtmine
Kehakaalu jälgimine ja kehamassiindeksi hindamine Uriinianalüüs Pööratakse tähelepanu paastuveresuhkru väärtusele ja hinnatakse gestatsioonidiabeedi riskitegureid.
Loode:
Loode kaalub nüüd oma platsentast rohkem. Loode kuuleb hääli ja haigutab. Moodustunud on rasunäärmed, millest eritunud rasu katab loote kaitsva lootevõidega.
Liigutused on koordineeritumad ja alluvad rohkem tahtele. Loode sirutab ja haarab. Igemed püsihammaste jaoks on moodustunud. Laps on võimeline tundma erinevaid maitseid. 20. nädalal on loode 25 sentimeetri pikkune ja kaalub 400 grammi.
Naine:
Esimese lapse ootuse ajal võib rase naine tunda loote liigutusi u 18.
nädalal, kuid selleks võib ka kuluda veel mõni nädal. Harjutusi tehes hingeldad ja higistad kergemini ning võid märgatavalt kaalus juurde võtta. See on tingitud muutustest ainevahetuses ja kilpnäärme aktiviseerunud talitlusest. Naba võib “välja punnitada”.
Mees:
Võimalusel koos osalemine loote anatoomia uurimise ultraheliuuringul, et olla kursis loote arenguga ja valmistuda isarolliks. Naine vajab sel ajal kedagi, kellega jagada nii rõõme kui muresid ja võimalikke hirme.
Mees saab naist toetada, hoidudes ka ise kahjulikest harjumustest ja pöörates tähelepanu tervislikule toitumisele ja liikumisele. Kodust toidulauda planeerides peaks meeles pidama, et lapseootel naine ei tohi süüa toorest liha ja kala, tooreid mune, pesemata köögi- ja puuvilju.
Listerioosi nakatumise vältimiseks mitte tarbida pastöriseerimata piima ja sellest tehtud piimatooteid.
Uuringud:
Arsti või ämmaemanda külastusel toimub naise kaalumine ja kaaluiive hindamine, jälgitakse tursete esinemist ja mõõdetakse vererõhku.
Üheks olulisemaks uuringuks raseduse ajal on looteanatoomia ultraheli (19.-21. nädalal).

Loode:
Loode kaalub umbes 450 grammi ja liigub aktiivselt. Tal on juba kulmud ja ripsmed. Loode on tõenäoliselt kõige aktiivsem siis, kui naine puhkab. Kasvavad esimesed tõelised juuksed.
Kaelalülid on selgelt nähtavad. 23. nädalal kaalub loode umbes 550 grammi. 23. nädalast on hea visualiseerida 4D ultraheliuuringu käigus loote näojooni.
24. nädalal on loode umbes 30 sentimeetri pikkune ja kaalub umbes 650 grammi.
Naine:
Võivad tekkida kõrvetised, mõned naised märkavad igemete paistetust.
Umbes sel ajal võivad avalduda emaka ebaregulaarsed kokkutõmbed.
Emakapõhi on tõusnud ja kõht kasvab jõudsalt. Loode reageerib erinevatele meeleoludele ja võib sündides ära tunda need laulud, mida naine raseduse ajal laulis. Loote liigutused tugevnevad.
Mees:
Mees saab aidata jälgida, kui naisel esineb peavalu, nägemishäireid, tugevat valu roidekaare all, korduvat oksendamist raseduse II või III trimestril ja käte ja näo tursete tekkimist ja vajadusel olla valmis pöörduma naisega tervishoiuteenuse osutaja poole.
Uuringud/tegevused:
- Emakapõhja kõrguse mõõtmine
- Loote südamelöökide kuulamine
- Soovi korral 4D ultraheliuuring (24.–32. nädal)
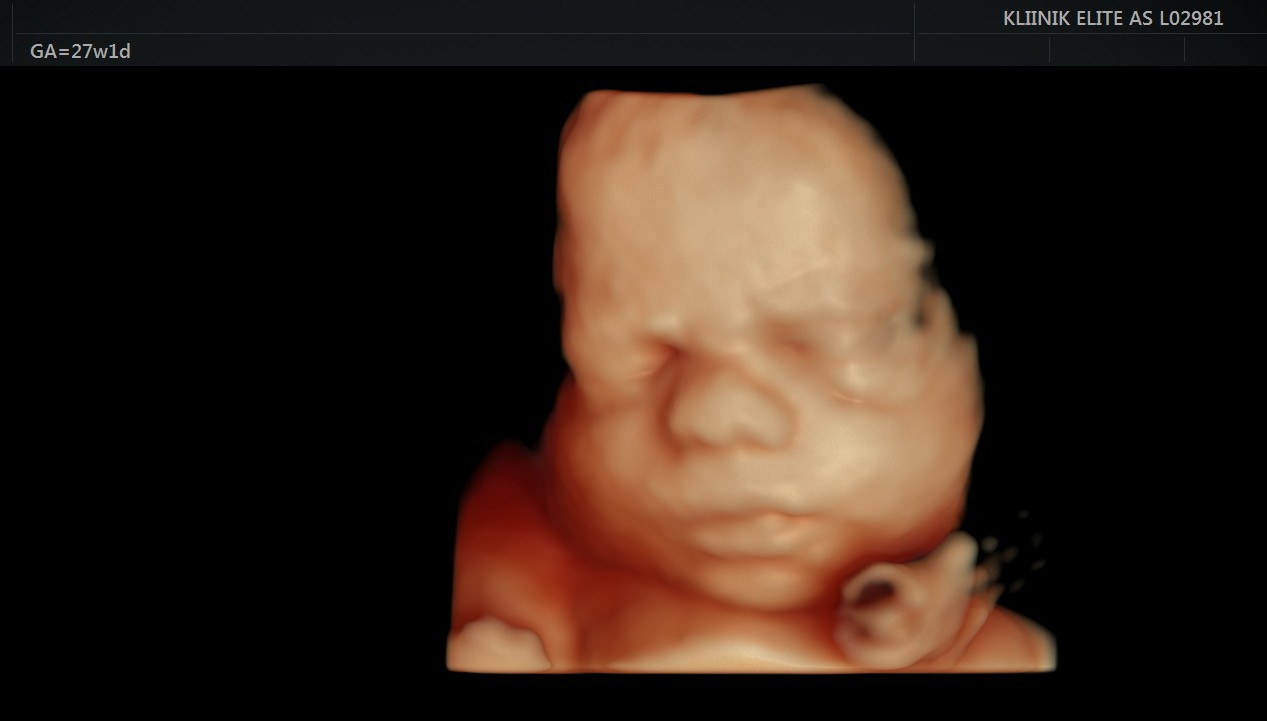
Loode:
Loote luud hakkavad tugevnema. Kopsudes moodustub aine, mis hingama hakkamisel aitab kopsudel avaneda. Loode teeb regulaarseid hingamisliigutusi. Loote nahk muutub vähem läbipaistvaks. Loote silmad reageerivad valgusele. Loote nahk on kortsuline ja tumepunane. Loote lõug muutub ümaramaks ning jalalaba suurus on umbes 2 sentimeetrit.
Loote kaal on umbes 1 kilogramm ja ta on 35 sentimeetri pikkune. See on parim aeg 4D ultraheliuuringu käigus loote näo vaatamiseks.
Naine:
Tavapärasest sagedamini võivad tekkida jalakrambid. Urineerimise vajadus sageneb. Rindadest võib pisut immitseda ternespiima ehk kolostrumit.
Mees:
See on aeg, mil võiks hakata tasapisi mõtlema sünnituse peale ja uurida, keda sooviks naine sünnitusele tugiisikuks. Sel ajal on võimalik koos käia ka 4D ultraheliuuringul, mis annab infot lapse tervise ja arengu kohta ning võimaldab tulevastel lapsevanematel jälgida reaalajas oma lapse tegevust, tekitades elevust ja pakkudes positiivseid emotsioone.
Uuringud:
- Vajadusel glükoositaluvuse test (24.-28. nädalal)
- Uriini- ja vereanalüüsid
- Naise kaalumine, kaaluiive hindamine
- Vererõhu ja emakapõhja kõrguse mõõtmine
- Tursete esinemise jälgimine
- Soovi korral 4D ultraheliuuring
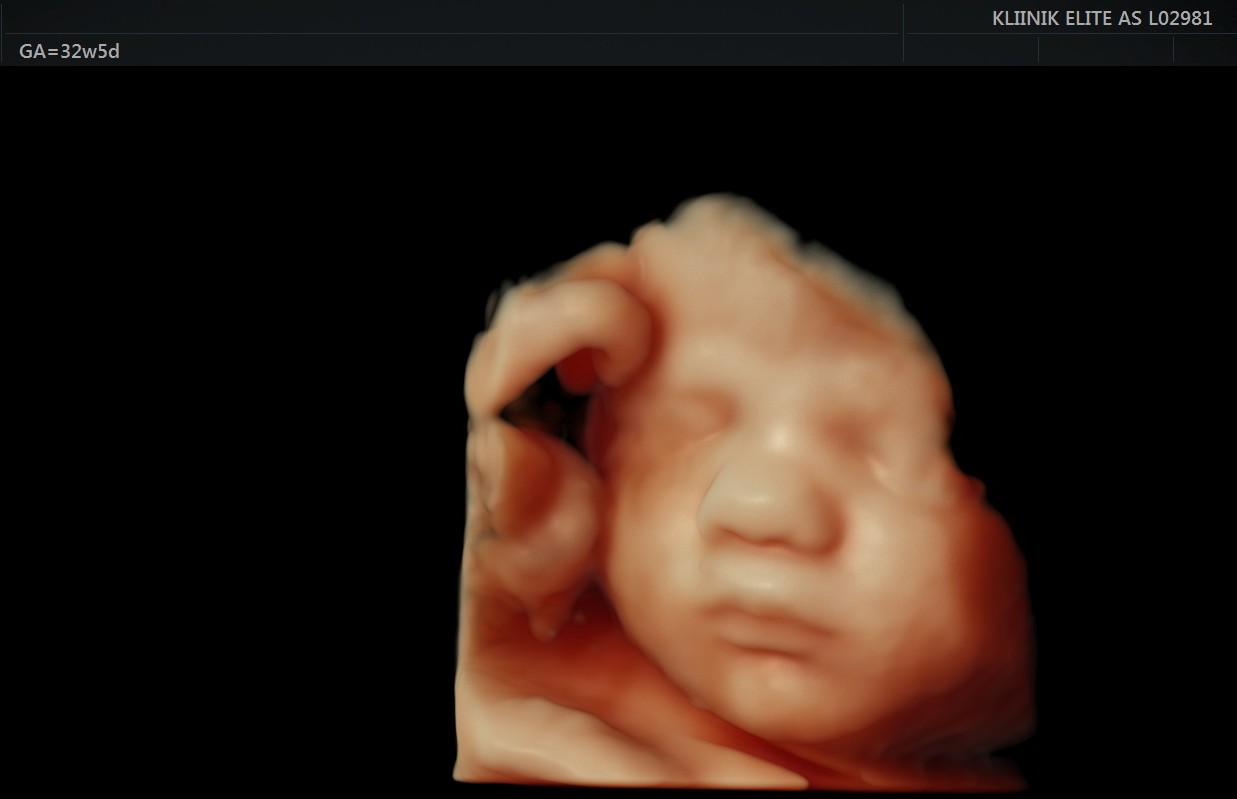
Loode:
Loode liigutab ja sirutab. Samuti oskab loode urineerida ning joob umbes
0,5 liitrit lootevedelikku päevas, mis väljub uriinina. Ta kaalub umbes
1,3 kilogrammi ja on 37 sentimeetri pikkune. Liigutades rindkeret harjutab loode hingamist. Loote kopsud on välja arenenud. 31. nädalal kaalub loode umbes 1,6 kilogrammi ja on 39 sentimeetri pikkune. Enamuse ajast ta magab. 32. nädalal on loode umbes 40 sentimeetrit pikk ning kaalub umbes 1,8 kilogrammi. Platsenta kaalub umbes 380 grammi.
Naine:
Loode surub naise soolestikule. Naine võib tunda emaka kokkutõmbeid.
Raske kõht võib naist vaevata ja trepist üles minnes ei jätku enam õhku.
Kehas on toimunud erinevad füsioloogilised muutused. Lapseootel töötav naine saab soovi korral jääda emapuhkusele 70 päeva enne lapse eeldatavat sünnitähtaega.
Mees:
Sellel perioodil vajab naine suurema tõenäosusega oma partneri tuge ja abi. Kätte on jõudnud ka aeg, mil ühiselt külastada perekooli. Elite kliinikus viib kogenud ämmaemand läbi individuaalset perekooli, kus on mugav tegeleda just nende teemadega, mis on hetkel paari jaoks aktuaalsed ja huvipakkuvad.
Uuringud:
Ultraheli ja erinevate analüüside vajalikkust hindab arst.
Loode:
Loode võib olla võtnud sisse pea alaspidi asendi. Süda lööb umbes
120-160 lööki minutis. Loode võib aeg-ajalt luksuda. Loote nahk on nüüd roosa. Loode eristab valgust ja pimedust ning kaalub umbes 2,2 kilogrammi. 35. nädalal kaalub loode umbes 2,5 kilogrammi. 36. nädalal on loode täiesti välja arenenud. Ta on umbes 45 sentimeetri pikkune. Pea läbimõõt on umbes 9 sentimeetrit.
Naine:
Nüüd võib naine aeg-ajalt tunnetada loote jalga või teisi kehaosasid.
Mõnedel rasedatel esinevad seljavalud. Liigesed, lihased ja sidemed muutuvad lõdvemaks.
Sageli jääb lapseootel naine emapuhkusele 30 päeva enne lapse eeldatavat sünnitähtaega. Normaalse raseduse korral lubatakse rasedaid lennureisile enamike lennufirmade poolt kuni 36. rasedusnädalani. Vajalik võib olla raseduse suurust ja sünnitustähtaega sisaldava dokumendi olemasolu. Pikkade reiside ajal suureneb venoosse trombemboolia risk, mistõttu on vajalik liikumine lennu ajal, tugisukad ja piisav vedeliku tarbimine.
Sel perioodil soovitatakse võtta osa perekooli loengutest. Elite kliinikus on soovijatele ka ämmaemanda individuaalne nõustamine, kus käsitletakse sünnituseks ettevalmistust ja vastsündinu eest hoolitsemist.
Mees:
Mees peab arvestama, et teatud juhtudel peab olema valmis enneaegseks sünnituseks või näiteks selliseks protseduuriks nagu loote väline pööramine (kui loode on tuharseisus). Naine vajab sel ajal mehe tuge ja abi. Kätte on jõudnud aeg valmistuda sünnituseks ja planeerida beebi saabumiseks vajalikud abivahendid.
Uuringud:
Loote eesasuva osa määramine (tuharseis) Ultraheliuuringu vajadust hindab arst, ultraheliuuring võimaldab hinnata loote oletavat kaalu, lootevee hulka, platsenta asukohta ja loote seisu, hoiakut, asetsust ja eesasuvat osa, visualiseerida loote strukturaalseid anomaaliad.
Uriinianalüüs
Vajadusel vereanalüüsid
Loote liigutuste jälgimine ja loote südamelöökide kuulatlemine Vajadusel kardiotokograafia
Loode:
Loote soolestik on täidetud esmasroojaga ehk mekooniumiga. 37. nädalal kaalub loode umbes 2,8 kilogrammi ja lootevett on umbes 1 liiter. 38. nädalast suureneb loote kaal kuni 30 grammi päevas. Lootevedelik uueneb iga 3 tunni järel. Loote nahk on roosa. Loode võtab nädalaga kaalus juurde 200-250 grammi. 40. nädalal on loote kaal on umbes 3-3,5 kilogrammi, pikkus umbes 50-53 sentimeetrit.
Naine:
Naise rasedust jälgiv ämmaemand või arst oskab öelda, kas lapse pea on vajunud vaagnapõhja. Sellel perioodil käib lapseootel naine arsti või ämmaemanda vastuvõtul iga kahe nädala järel. Naine võib tunda loote pead vaagnapõhja vastas ja täheldada, et ta liigutab vähem. Lapseootel naise emakakael muutub pehmeks ja naine võib tunda ennast väga raskelt, raskusi võib olla ka magamisasendi leidmisega. Sünnitus läheneb. Loote pea pressib pehmenenud emakakaela vastu ja naine on füsioloogiliselt sünnituseks valmis.
Mees:
Sel perioodil peab olema valmis, et naisel võib igal hetkel alata sünnitustegevus. On aeg kokku leppida, kas eelistatakse peresünnitust.
Eestis on võimalik kasutada isapuhkust, kätte on jõudnud õige aeg soovi korral see planeerida.
Uuringud:
- Uriinianalüüs
- Vajadusel vereanalüüsid
- Ultraheliuuring alates 36. nädalast
- Vajadusel kardiotokograafia ehk KTG